

How Do You Diagnose Sex Addiction?
Sex Addiction is quite controversial. At Restored Life, this is one of our specialties. The best answer to this question requires a bit of context.
Article Topics

- The most common symptoms of sex addiction.
- Why the most common criticisms of diagnosing and treating sex addiction are flawed.
- How we diagnose sex addiction or porn addiction here at Restored Life.
- The politics surrounding sexual addiction as a clinical problem. (And which hinder effective diagnosis by non-specialist clinicians).
The Most Common Symptoms of Sexual Addiction

This is most likely what you’re here for. So I’ll address it first. But I encourage you to read the rest of the article to put this information in context.
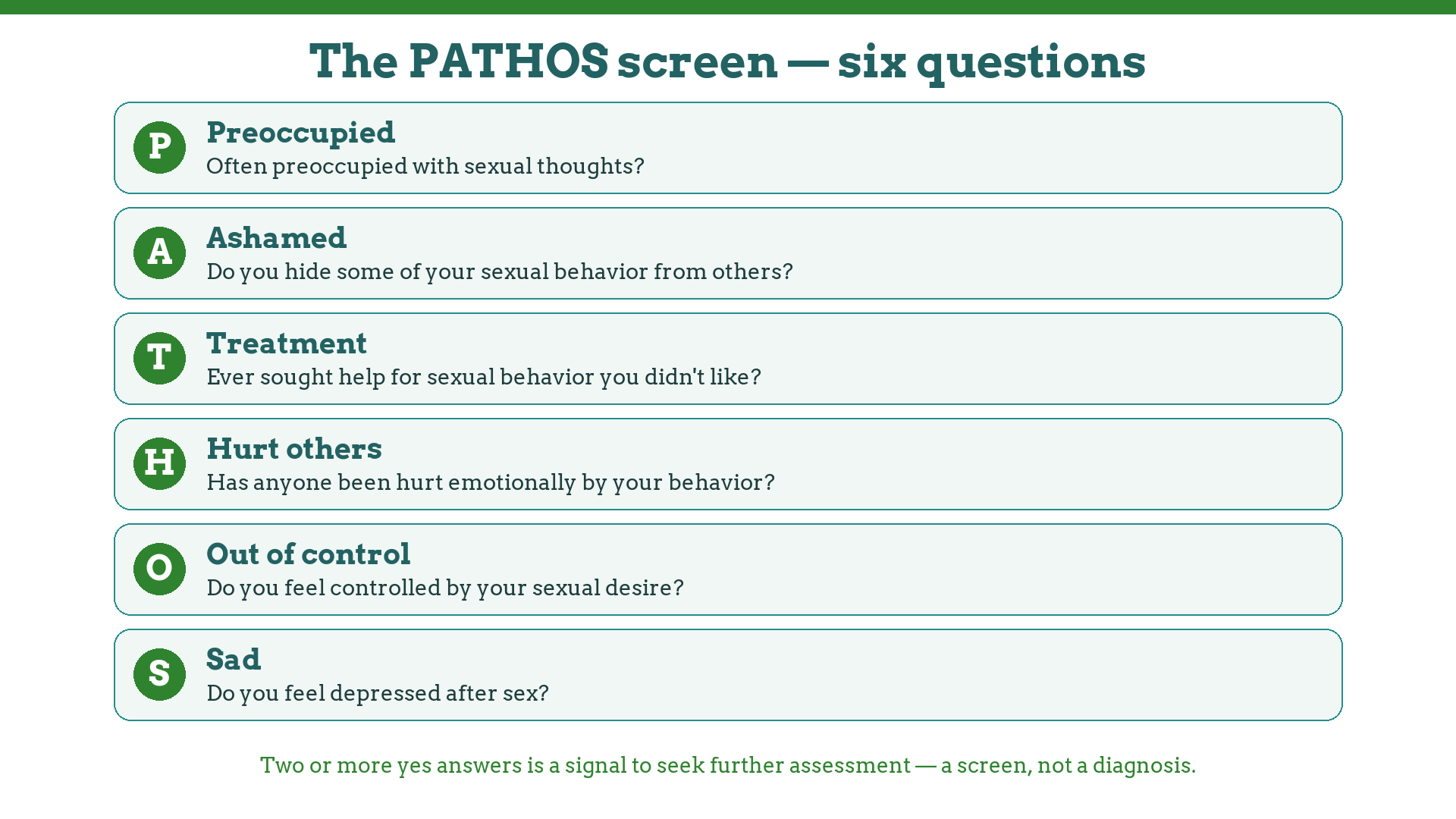
A brief screening tool for sex addiction is the PATHOS survey. This is NOT a definitive diagnosis, but a signal that it may be wise to seek help. This is also not a full list of diagnostic criteria, but it is a good place to start. There are six yes or no questions on the PATHOS survey. If you answer, “yes,” to two or more, it may be wise to seek a further assessment.
- Do you often find yourself preoccupied with sexual thoughts? [Preoccupied]
- Do you hide some of your sexual behavior from others? [Ashamed]
- Have you ever sought help for sexual behavior you did not like? [Treatment]
- Has anyone been hurt emotionally because of your sexual behavior? [Hurt others]
- Do you feel controlled by your sexual desire? [Out of control]
- When you have sex, do you feel depressed afterward? [Sad]
A modified version of the PATHOS survey is included in our Personal Challenges Survey (PCS). The PCS includes brief screens for many challenges. This helps to understand each challenge in context. We recommend this wide-spectrum approach over a single-issue brief screening. The PCS takes about 15 minutes to complete and is our proprietary recommendation for a sex addiction survey.
Each challenge on the PCS uses a 0-5 scale. Challenges scoring 2 or higher show that seeking professional help may be wise. Three or more challenges in the 1-2 range show that seeking professional help may be wise. With Restored Life, the first step to getting help is to visit our Get Started page and follow the instructions there.
Why Diagnose Sex Addiction or Porn Addiction?

Most simply, getting a proper diagnosis helps create the most helpful recovery plan. The most helpful plan then creates hope for something better. No diagnosis, no plan. No plan, no hope.
Most Common Criticisms of Diagnosing and Treating Sex Addiction

As I stated above, this issue is controversial. There are many criticisms therapists who diagnose and treat sex addiction. Most critics claim that the whole field is invalid and wrong.
Yet, there is much to gain if we engage with our critics instead of ignoring them or raging against them. Most of these criticisms actually provide some good ethical guard rails. These guard rails are actually good for us and for our clients.
Is there a financial motive to over-diagnose sex addiction?
Treating sex addiction is one of our specialties here. But it is not our only specialty. And not all our clients are here for help with our specialty issues. There is plenty of work to do even if we had zero clients for sexual addiction.
Over-diagnosing sex addiction would actually put us out of business. No one wants this label. It carries an unbelievable amount of stigma. If we over-diagnose this issue, we would be harming our clients. Harming our clients would lead to ethics complaints, lawsuits, and negative clinical outcomes. Any of those problems would put us out of business.
This “financial motive” criticism has happened for every “new” psychological diagnosis. It happened for Post Traumatic Stress. Psychotherapy as a field has been subjected to this criticism for its entire history.
There is nothing wrong with getting paid for helping people overcome their problems. There is something wrong with making clients dependent upon therapy. to have a healthy and fulfilling life.
Our goal is always to graduate clients from therapy to community-stable-sobriety. (I’ll write about what I mean by this in a future article).
How do you honor diverse sexual values when diagnosing sex addiction?
There is a wide range of sexual values in our society. From conservative and religious sexual values to liberal and permissive sexual values. Both ends of the spectrum criticize people who research, diagnose, or treat sex addiction.
On the conservative religious end… there is a desire to frame sexual addiction from a purely moral perspective. Only certain, if any, sexual behavior is acceptable. The belief is that diagnosis removes one’s responsibility for their choices and behavior. This is not true.
If this criticism were true, then we would not charge drunk drivers with DUI’s. In reality, diagnosis empowers one to take responsibility for their recovery. Diagnosis also helps the helpers have greater compassion for their clients.
On the liberal and permissive end… the “sex-positive” movement… there is a desire to not moralize or pathologize any sexual behavior or relationship. One belief is that diagnosis is inherently shameful. Another belief is that the diagnosis of sex addiction robs all joy from sex.
If this criticism were true, then we would have to revisit and redefine every diagnosis in modern healthcare. On the contrary, diagnosis connects one to a recovery community. This connection to the community reduces shame. Further, it increases the joy available from healthy sex. It loosens the controlling grip that sexual behavior has had in the person’s life until now.
Any diagnosis of any condition must honor the client’s or patient’s values. Treatment must help that person live more with integrity with their stated values. This is not unique to the field of sex addiction treatment. But it is rarely thought of in other health fields.
Restored Life’s Sexual Values
Healthy sex should be a source of:
- intimacy,
- connection,
- erotic exploration,
- play,
- joy,
- comfort,
- and fulfillment
- for consenting adults.
Healthy sex may or may not always lead to procreation. Sex should never be the sole source of these things in anyone’s life. If sex is the sole source of these things, it will become an addiction.
Unhealthy sex is:
- any sex without consent;
- involving any degree of force, coercion, manipulation, or exploitation.
Sex with minors or children is morally abhorrent, illegal, and unhealthy. Minors and children are developmentally incapable of consent.
Sex between minors is best addressed from a sexual risk management perspective.
Comprehensive sex education represents one end of the spectrum of sexual values. It is more harmful than helpful.
Abstinence-only sex education represents one end of the spectrum of sexual values. It is more harmful than helpful from a clinical perspective.
Morally speaking, since Restored Life Counseling is a Christian Counseling center and holds traditional Christian values on marriage and sexuality, abstinence from any extramarital sex is what we advocate for in terms of behavior. Abstinence as the behavioral goal does not mean that abstinence-only sex education is helpful, even from a moral perspective.
How do you manage or prevent partner triangulation when diagnosing sex addiction?
Many are unclear on the sexual values, appetites, or preferences of both individuals in a relationship. This often causes strife in the relationship and often ends up with the couple in therapy.
Untrained therapists may side with one client or the other. This creates a “triangulation.” The therapist and “good partner” are on one side, and the “bad partner” on the other. This is harmful to couples and individuals. It is also unethical of the therapist.
Even with training, all therapists also hold sexual values. (We are not valueless and empty, we’re people, too).
Triangulation may happen when:
- The therapist has experienced porn addiction, sex addiction, infidelity, or betrayal trauma.
- The therapist holds sexual values different than one of the partners.
Triangulation against the partner with the addiction is likely when the therapist…
- Holds sexually conservative or religious values.
- Has experienced infidelity or betrayal trauma.
- Uses moral language against the partner with the addiction.
- Encourages the suppression of sexual behaviors.
- Encourages the change of sexual values.
If triangulation occurs, the partner with addiction may feel:
- Unheard
- Misunderstood
- Shamed
- Unsupported
- Dishonored
Triangulation against the betrayed partner is likely when the therapist…
- Holds sexually liberal-permissive values
- Has experienced sex addiction, porn addiction, or sexual trauma
- Uses moral language against the betrayed partner
- encourages more or new sexual behaviors
- encourages the change of sexual values
If triangulation occurs, the betrayed partner may feel:
- Unheard
- Misunderstood
- Shamed
- Unsupported
- Dishonored
A therapist who is trained to treat these issues may not be perfect at managing partner-triangulation. But they are generally better at it. I often frame this issue for my clients as a tightrope that we all have to walk on together. It is very easy to fall of either side. Falling of on either side may harm one partner or the other.
Hypersexuality vs. Compulsive Sexual Behavior vs. Sex Addiction vs. Value Incongruence

Over time, several different diagnostic labels for these issues have been proposed. There is a case for each of them. CSBD (described below) is in the list of mental disorders in the ICD-11. The DSM does not yet include any category for sex addiction. This means that insurance will not cover treatment for sexual addiction per se. There are legitimate ways to get insurance to cover your treatment, which I will discuss in another article.
Hypersexuality, or Hypersexual Disorder
This label is sometimes used interchangeably with the other proposed labels for this issue. But it is mostly used for excessive or unusual sexual behavior that is part of another mental disorder. For example, hypersexuality is a common symptom of bipolar disorder during a manic episode.
Hypersexuality may also be used when one partner in a relationship has a much higher sex drive than their partner.
Compulsive Sexual Behavior Disorder (CSBD)
This label was introduced in the ICD-11 in June of 2018. This makes CSBD the most acceptable label in clinical and research communities.
The ICD-11 entry for CSBD is “…characterized by a persistent pattern of failure to control intense, repetitive sexual impulses or urges resulting in repetitive sexual behaviour. Symptoms may include repetitive sexual activities becoming a central focus of the person’s life to the point of neglecting health and personal care or other interests, activities and responsibilities; numerous unsuccessful efforts to significantly reduce repetitive sexual behaviour; and continued repetitive sexual behaviour despite adverse consequences or deriving little or no satisfaction from it. The pattern of failure to control intense, sexual impulses or urges and resulting repetitive sexual behaviour is manifested over an extended period of time (e.g., 6 months or more), and causes marked distress or significant impairment in personal, family, social, educational, occupational, or other important areas of functioning. Distress that is entirely related to moral judgments and disapproval about sexual impulses, urges, or behaviours is not sufficient to meet this requirement.” (ICD-11)
Compulsive behavior is a sub-component of any addiction. So the inclusion of CSBD in the ICD-11 as a step in the right direction, but it may not go far enough.
Addiction expands on compulsive behavior by adding concepts of tolerance and withdrawal.
Sex Addiction
This label includes everything described in CSBD, as well as tolerance and withdrawal. Tolerance in sex addiction may look like this:
- an increased frequency of compulsive sexual behavior,
- or an escalation in the risk, shame, or even criminality* associated with the compulsive sexual behavior.
Withdrawal coincides with a reduction in sexual behavior, and may
look like:
- depression,
- anxiety,
- or an increase of non-sexual compulsive or addictive behavior.
*The significant majority of people struggling with sex addiction are not sex offenders. But most sex offenders are also struggling with sex addiction. Sex offender treatment is different from sexual addiction treatment. Restored Life does not provide sex offender treatment.
Value Incongruence
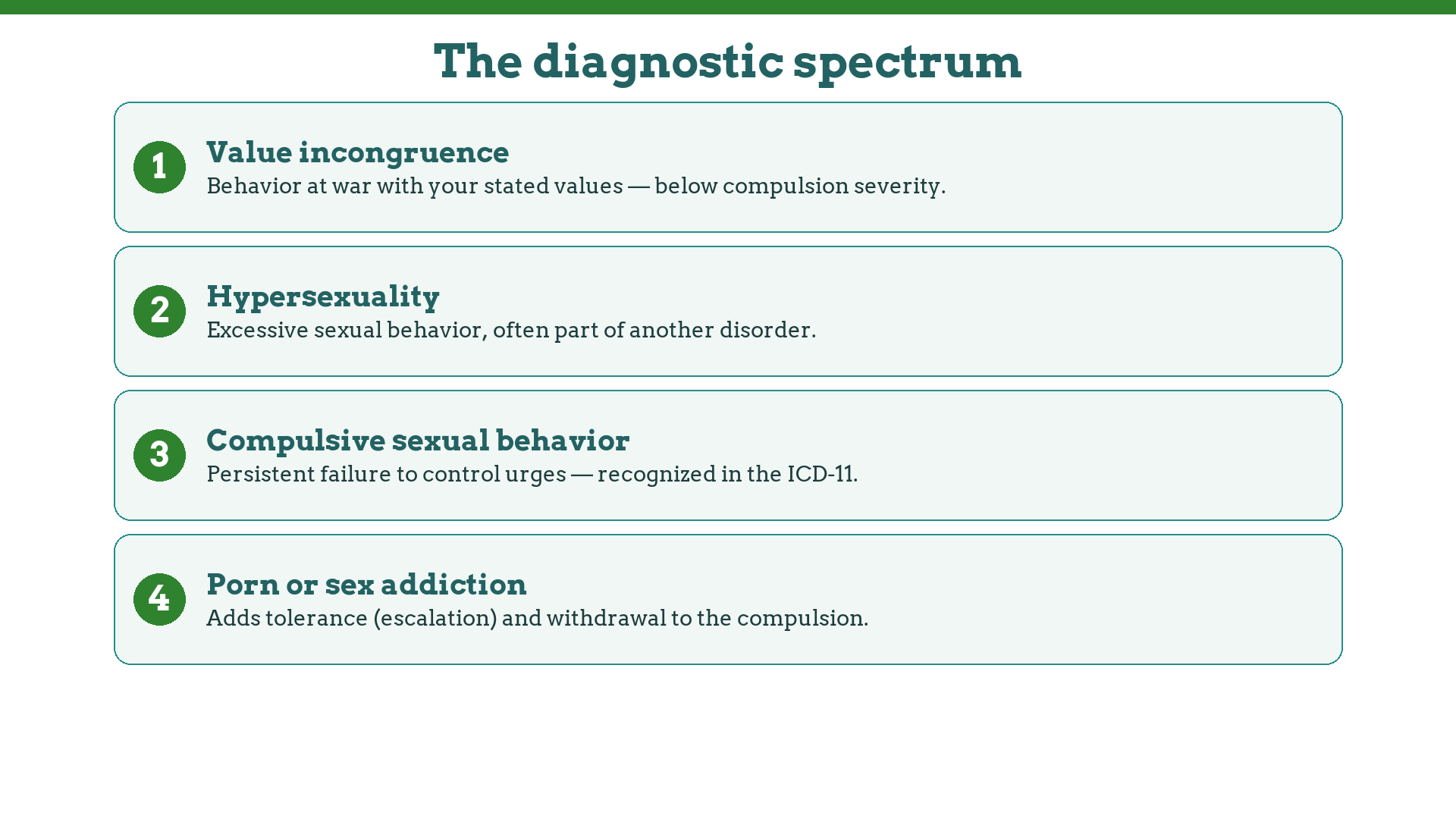
This is a recent label for repetitive sexual behavior that goes against a person’s stated values. But it does not rise to the severity of a compulsion or addiction to that behavior.
A Diagnostic Spectrum
Rather than treating the above labels as competing names for the same problem, it may be more helpful to put them on a spectrum.
The spectrum starts with value incongruence. Then hypersexuality. Then compulsive sexual behavior. Then porn or sex addiction.
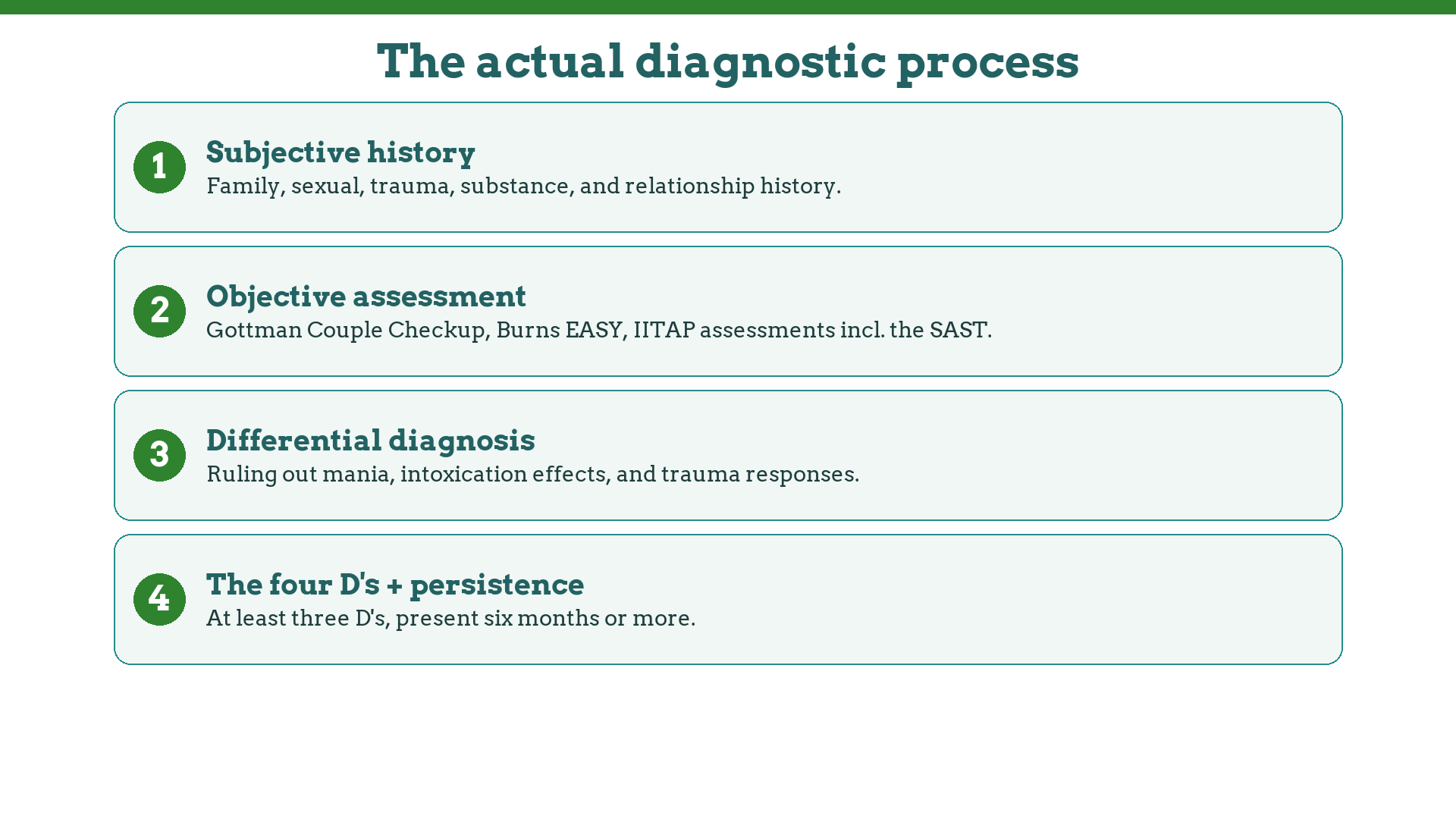
The Actual Diagnostic Process
Subjective History Gathering
Intake sessions cover several areas of personal history relevant to the presenting concern:
- family history,
- sexual history,
- trauma history,
- substance use history,
- relationship history,
- and other areas as time allows.
Objective Clinical Assessment
Couples will complete the Gottman Couple Checkup. This consists of 480 questions about the state and history of their relationship. Individuals will complete the David Burns EASY, and at least one assessment from IITAP. These are well-researched clinical assessments with high reliability and validity. Their validity increases when used together. And their validity increases even more with the subjective history taking described above.
The Carnes SAST (included in the IITAP assessments) has several subscales that can be used to line up with each of the diagnostic labels above. In this sense, the SAST is the most complete symptom list of any current screening tool for sex addiction. The SAST is not a list of diagnostic criteria. Diagnostic criteria and symptoms are not the same things.
Differential Diagnosis – Discerning Sex Addiction from Other Mental Health Issues
Some mental health problems have hypersexuality as one of their symptoms. For example, hypersexuality is common during manic episodes for people with bipolar disorder. If hypersexuality persists outside of manic episodes, then sexual addiction may be present.
Unwanted or value-incongruent sexual behavior may also occur when intoxicated. Sexual behaviors may be an unwanted side effect of using intoxicants. Or, intoxicants may be used to enable sexual behavior that one would not do otherwise.
Hypersexuality is also common for people with a history of sexual trauma. There may be a “cathartic” purpose in one’s sexual behavior. Or, seeking cathartic sexual experiences may become a controlling principle in one’s life. Re-enacting sexual experiences like one’s sexual trauma may be either cathartic or re-traumatizing. So context and impact play a huge role in differential diagnosis.
These are only a few examples where differential diagnosis is in play. Every client is unique. No label is applied only because a person checks (or does not check) the right boxes in a survey. Every client’s personal values and unique experiences are considered in the diagnostic process.
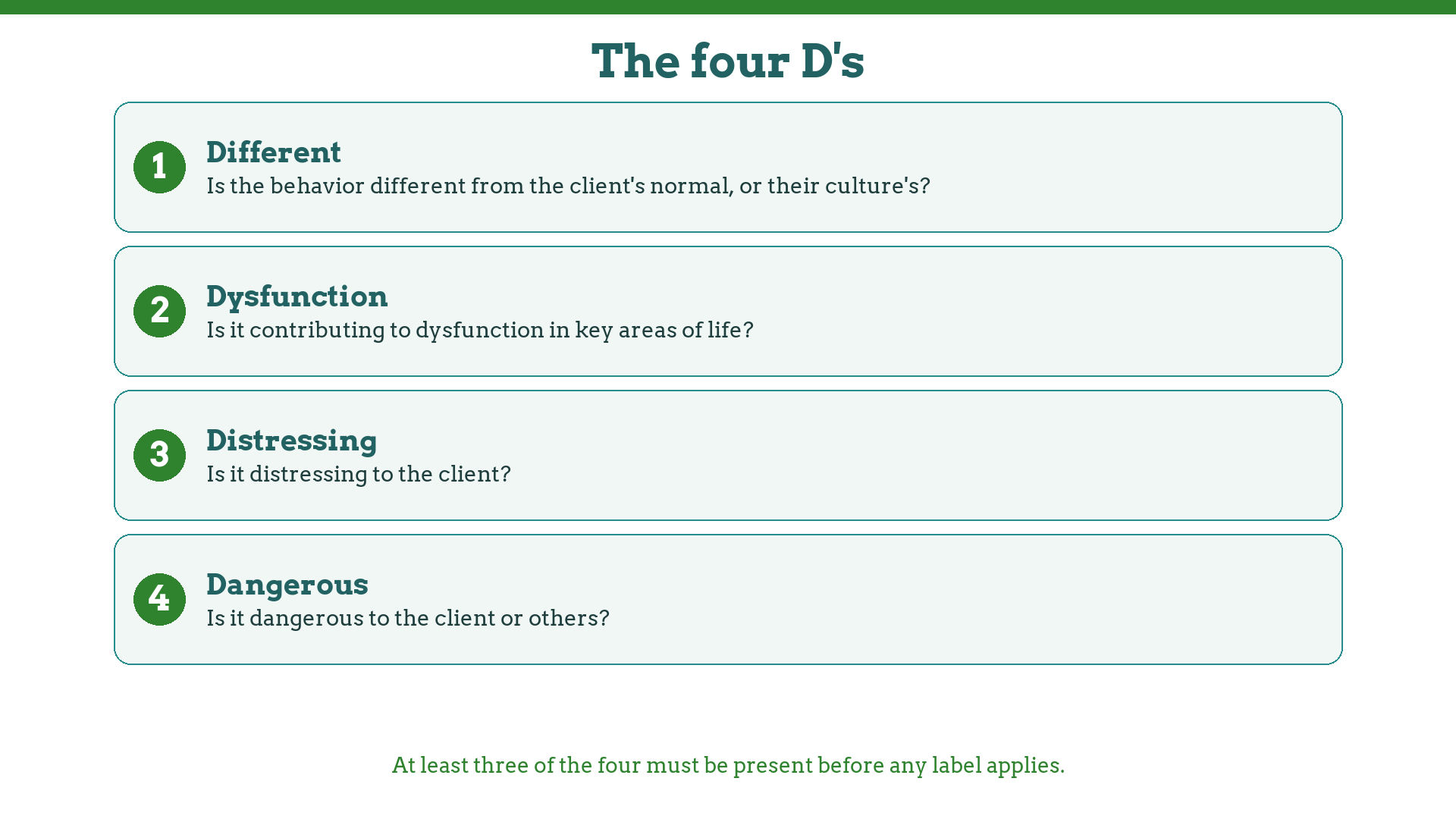
The Four D’s
All the labels on the spectrum of sex addiction include certain behaviors. These behaviors may be problematic. But, some of those behaviors may be “normal,” and even healthy in certain contexts. (For example, a young couple trying to get pregnant will naturally have increased sexual activity). So our final step before applying any label to a client’s behaviors is to consider “the 4 D’s.” If at least three of the 4 D’s must be present.
- Is the behavior or symptom different than normal for the client or the client’s culture?
- Is the behavior or symptom contributing to dysfunction in key areas of the client’s life?
- Is the behavior or symptom distressing to the client?
- Is the behavior or symptom dangerous to the client or others?
Summary
A label on the spectrum of sex addiction may apply if:
- A client’s personal history shows contributing factors.
- A client’s symptom survey responses support applying the label.
- A client’s symptoms are not better explained by another health condition.
- A client’s symptoms and situation include at least three of the four “D’s.”
- A client’s symptoms and pattern of behavior have persisted for six months or more.
Save and share
Pin or share these — someone you love may need them today.
References
- Kraus, S. W., Krueger, R. B., Briken, P., et al. (2018). Compulsive sexual behaviour disorder in the ICD-11. World Psychiatry, 17(1), 109–110. https://doi.org/10.1002/wps.20499
- Kraus, S. W., Voon, V., & Potenza, M. N. (2016). Should compulsive sexual behavior be considered an addiction?. Addiction, 111(12), 2097–2106. https://doi.org/10.1111/add.13297
- Reid, R. C., Carpenter, B. N., Hook, J. N., et al. (2012). Report of findings in a DSM-5 field trial for hypersexual disorder. Journal of Sexual Medicine, 9(11), 2868–2877. https://doi.org/10.1111/j.1743-6109.2012.02936.x
- Carnes, P., Green, B., & Carnes, S. (2010). The same yet different: Refocusing the Sexual Addiction Screening Test (SAST) to reflect orientation and gender. Sexual Addiction & Compulsivity, 17(1), 7–30. https://doi.org/10.1080/10720161003604087
- Bőthe, B., Potenza, M. N., Fuss, J., et al. (2021). The development of the Compulsive Sexual Behavior Disorder Scale (CSBD-19): An ICD-11 based screening measure across three languages. Journal of Behavioral Addictions, 9(2), 247–258. https://doi.org/10.1556/2006.2020.00034